Case history
A middle-aged female with a past medical history of diabetes and end stage renal disease resulting in kidney transplant presented for evaluation of right hip and knee pain for the previous two months. An MRI of the hip revealed a large effusion with evidence of septic arthritis, myositis in the surrounding muscle, and osteomyelitis of the hip. Blood cultures remained negative for the duration of her presentation. The patient underwent a joint aspiration, and synovial fluid was sent to the microbiology laboratory for culture. Due to subsequent culture positivity and the extent of the involvement of the surrounding anatomy, the patient was started on ceftriaxone and underwent a total joint replacement. Her symptoms improved post-procedure, and post-operative vertebral MRI and TTE revealed no evidence of osteomyelitis or endocarditis. The patient was discharged on post-operative day six with continued IV ceftriaxone for an additional 5 weeks.
Laboratory identification
The synovial fluid received in the microbiology laboratory was plated onto blood, chocolate, and MacConkey agars. No organisms were visible on direct Gram stain, but the culture revealed scant growth of alpha-hemolytic colonies on blood and chocolate plates. These colonies were comprised of faintly staining gram positive rods (Image 1). The organism was catalase negative. Given the characteristic appearance by Gram stain, the organism was inoculated to a triple sugar iron (TSI) slant where it demonstrated H2S production. A definitive identification of Erysipelothrix rhusiopathiae was achieved by MALDI-TOF MS.

Discussion
Erysipelothrix rhusiopathiae is a facultatively aerobic, non-spore forming, gram positive pathogen that is a resident of the digestive and respiratory tracts of mammals, bird, fish, and pigs.1 It is the etiological agent of Swine Erysipelas, causing either an acute septicemia, cutaneous disease, endocarditis, or chronic arthritis in pigs. Human infections with E. rhusiopathiae are usually due to exposure to infected animals or contaminated animal products or environments. Certain occupations with frequent animal exposure are at increased risk for infection (including fishermen, veterinarians, farmers, and butchers). Infection requires entry into the skin through cutaneous abrasions, which can be caused by sharp hooks, fish scales, teeth, and other occupational tools or hazards that damage epithelial barriers.1,2
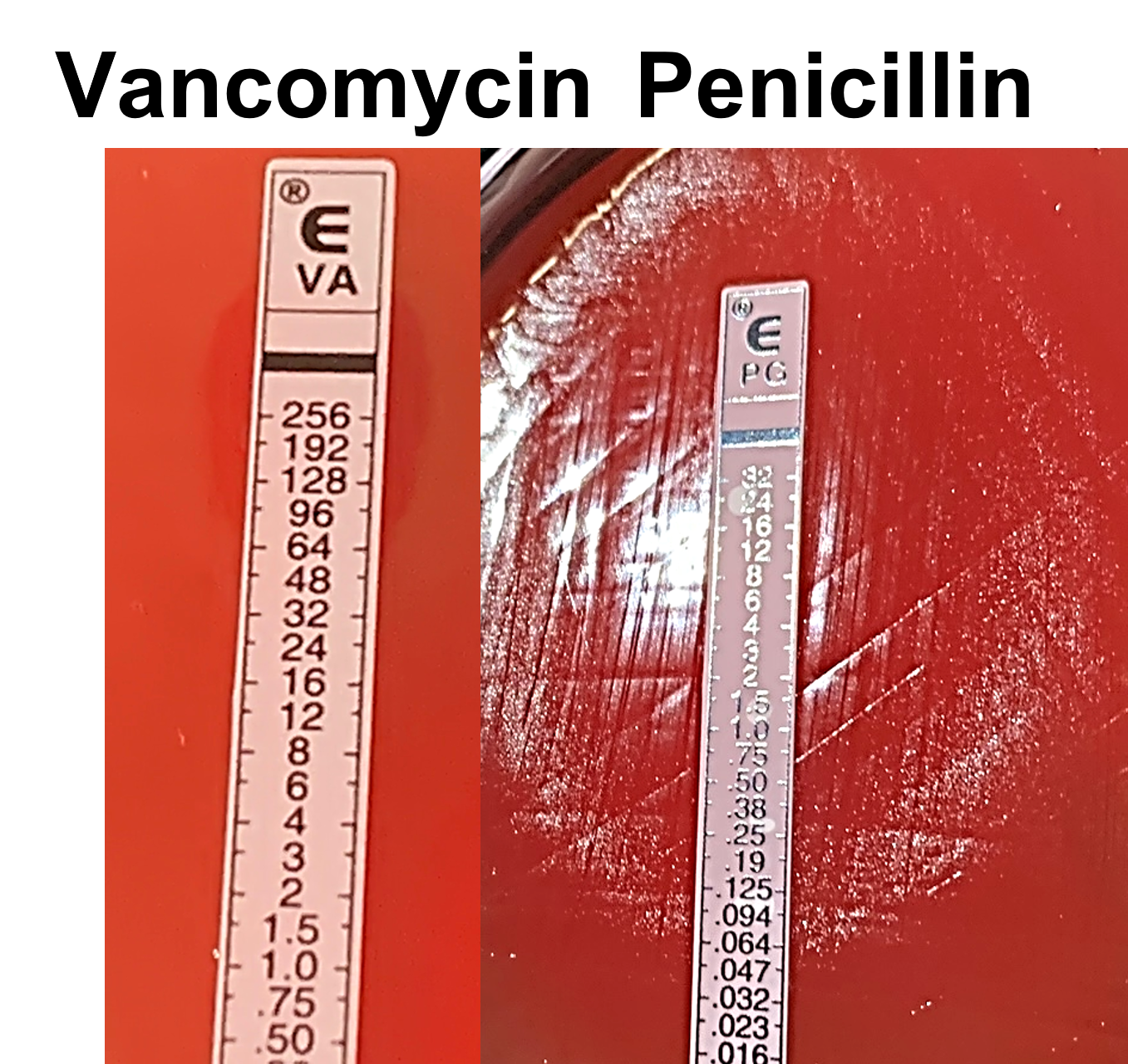
Human E. rhusiopathiae infection can manifest as three distinct forms. An acute, localized cellulitis named eryspieloid (not to be confused with streptococcal erysipelas) is the most common manifestation. This usually impacts the hands, fingers, or other parts of the upper extremities that have contact with animals or animal products.3 A generalized cutaneous form more often associated with systemic symptoms including fever, joint aches, lymphadenitis, lymphadenopathy, and arthritis can also occur. Finally, septicemia frequently associated with endocarditis is a third manifestation. E. rhusiopathiae endocarditis is often subacute, with a tropism for native valves (particularly the aortic valve). Due to its indolent nature, this presentation often requires valve replacement at the time of diagnosis and is associated with increased mortality.1,4 While cases of non-severe eryspieloid may self-resolve, ampicillin or penicillin are the treatments of choice for cutaneous and systemic infections. Cephalosporins and fluoroquinolones are also efficient alternative agents.3 Importantly, the organism is intrinsically resistant to vancomycin, thus accurate and timely identification is critical to ensure appropriate intervention (Image 2). Susceptibility testing is generally not performed but may be useful in the setting of penicillin allergy.
Laboratory identification of E. rhusiopathiae can be challenging. Erysiepelothrix can easily decolorize during gram staining and can be mistaken as gram negative due to lack of stain retention. Additionally, the cells can exhibit variable morphologies including pairs, chains, and filaments. Colonies can also exhibit variable morphotypes when grown on routine media, including both rough and smooth forms.2An environmental exposure to animals was investigated in this patient’s case to possibly serve as the source of infection. While a direct link cannot be definitively proven, it was revealed that the patient owned a large fish tank which she regularly cleaned which could have been a potential source of infection.
References
- Wang Q, Chang BJ, Riley TV. 2010. Erysipelothrix rhusiopathiae. Veterinary Microbiology 140:405-417.
- Clark AE. 2015. The Occupational Opportunist: an Update on Erysipelothrix rhusiopathiae Infection, Disease Pathogenesis, and Microbiology. Clinical Microbiology Newsletter 37:143-151.
- Veraldi S, Girgenti V, Dassoni F, Gianotti R. 2009. Erysipeloid: a review. Clinical and Experimental Dermatology 34:859-862.
- Brooke CJ, Riley TV. 1999. Erysipelothrix rhusiopathiae: bacteriology, epidemiology and clinical manifestations of an occupational pathogen. Journal of Medical Microbiology 48:789-799.

-Timothy J. Kirtek, M.D., originally from Grand Blanc, Michigan, graduated from American University of the Caribbean School of Medicine located on the island of Sint Maarten. There, he conducted research on tropical arboviruses including Dengue, Chikungunya, and Zika viruses. He then returned to Michigan to complete his clinical training and, upon graduation from medical school, moved to Dallas, Texas where he is currently an Anatomic and Clinical Pathology resident physician at UT Southwestern.

-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern Medical Center in the Department of Pathology, and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.

This is informative
Thank you very much