History
Miliaria crystallina
This form usually affects neonates younger than 2 weeks and adults who are febrile or those who recently moved to a tropical climate.
Lesions appear in crops within days to weeks of exposure to hot weather and disappear within hours to days.
Lesions are generally asymptomatic.
Miliaria rubra
This form usually affects neonates aged 1-3 weeks and adults who live in hot, humid environments.
Lesions may occur under transdermal medication patches. [3]
Lesions may occur within days of exposure to hot conditions, but they tend to appear after months of exposure.
Lesions resolve within days after the patient is removed from the hot, humid environment.
Lesions cause intense pruritus and stinging that is exacerbated by fever, heat, or exertion.
Patients may report fatigue and heat intolerance, and they may notice decreased or absent sweating at the affected sites.
Miliaria profunda
This form occurs in individuals who usually live in a tropical climate and have had repeated episodes of miliaria rubra.
Lesions develop within minutes or hours after the stimulation of sweating. These lesions resolve quickly, usually in less than an hour after the stimulus that causes sweating is removed.
The lesions are asymptomatic.
Patients may report increased sweating in unaffected skin; swollen lymph nodes; hyperpyrexia; and symptoms of heat exhaustion, which include dizziness, nausea, dyspnea, and palpitations.
A rare giant centrifugal variant of miliaria profunda has been reported in 2 infants, each at about age 3 months, who presented with symmetrical asymptomatic lesions on the trunk and extensor extremities after a low-grade fever. Unlike most forms of miliaria, the lesions in these children persisted for months. [27]
Physical Examination
Miliaria crystallina
Lesions are clear, superficial vesicles that are 1-2 mm in diameter.
Lesions occur in crops and are often confluent, without any surrounding erythema.
In infants, lesions tend to occur on the head, neck, and upper part of the trunk.
In adults, lesions occur on the trunk.
Lesions rupture easily and resolve with superficial branny desquamation.
See the images below.
 Miliaria crystallina in an infant. Note that the lesions are confluent. Courtesy of K.E. Greer, MD.
Miliaria crystallina in an infant. Note that the lesions are confluent. Courtesy of K.E. Greer, MD.

 Miliaria crystallina. Note the water-drop appearance of the lesions. Courtesy of K.E. Greer, MD.
Miliaria crystallina. Note the water-drop appearance of the lesions. Courtesy of K.E. Greer, MD.
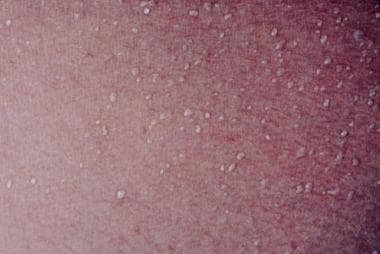
Miliaria rubra
Lesions are uniform, small, erythematous papules and vesicular papules on a background of erythema.
Lesions occur in a nonfollicular distribution and do not become confluent.
In infants, lesions occur on the neck and in the groin and axillae.
In adults, lesions occur on covered skin where friction occurs; these areas include the neck, scalp, upper part of the trunk, and flexures. The face and volar areas are spared.
Lesions may occur in erythematous patches similar to sunburn. [28]
In late stages, anhidrosis is observed in affected skin.
See the image below.

Miliaria profunda
Lesions are firm, flesh-colored, nonfollicular papules that are 1-3 mm in diameter.
Lesions occur primarily on the trunk, but they can also appear on the extremities.
Lesions are transiently present after exertion or other stimulus that results in sweating.
Affected skin shows diminished or absent sweating.
In severe cases that lead to heat exhaustion, hyperpyrexia and tachycardia may be observed.
A rare giant centrifugal variant of miliaria profunda has been reported in young infants (of about age 3 mo) who presented with multiple erythematous lichenoid papules that coalesced to form infiltrated annulare and geographic plaques 1-5 cm in size with an erythematous border, located over the trunk and extensor extremities. [27]
Complications
The most common complications of miliaria are secondary infection and heat intolerance.
Secondary infection may appear as impetigo or as multiple discrete abscesses known as periporitis staphylogenes.
Heat intolerance is most likely to develop in patients with miliaria profunda; it is recognized by anhidrosis of the affected skin, weakness, fatigue, dizziness, and even collapse. In its most severe form, this heat intolerance is known as tropical anhidrotic asthenia.
-
Miliaria crystallina in an infant. Note that the lesions are confluent. Courtesy of K.E. Greer, MD.
-
Miliaria rubra in an adult. Courtesy of K.E. Greer, MD.
-
Miliaria pustulosa. Courtesy of K.E. Greer, MD.
-
Miliaria crystallina. Note the water-drop appearance of the lesions. Courtesy of K.E. Greer, MD.
-
Miliaria crystallina in a newborn child. Courtesy of K.E. Greer, MD.
-
Miliaria pustulosa. Courtesy of K.E. Greer, MD.







